
Research Article | DOI: https://doi.org/10.31579/2690-8794/047
*Corresponding Author: Alfateh Sayed M. Noor, Critical Care Department, King Saud Medical City, Riyadh, KSA.
Citation: Alfateh S. M. Noor, Alharthy A., Mohammed H. Lhmdi, Elshareef H. , Farea Z., Bokhamseen Md., Mhawish H., Waleed Th. Aletreby, Balhamar A., Ahmed F. Mady, (2020) Evaluating the impact of audit interventions on accidental removal of critical care devices in the intensive care unit - Clinical Audit Project J, Clinical Medical Reviews and Reports. 2(7); DOI: 10.31579/2690-8794/047
Copyright: © 2020, Alfateh Sayed M. Noor, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 September 2020 | Accepted: 02 October 2020 | Published: 05 October 2020
Keywords: ICU; critical care devices; accidental removal; patient management
Accidental critical care device removals in intensive care units (ICUs) are serious preventable incidents that have major implications. The study aimed to understand possible causes of such events and identify interventions that reduced their occurrence. The researchers conducted a single-center audit by collecting patient data and bundle forms for accidental device removal across two consecutive periods; they retrospectively reviewed the data from the first period (August 1, 2019 to January 31, 2020) and prospectively analyzed the data from the bundle forms obtained in the second (February 1, 2020 to July 31, 2020). From the findings of the first period, the researchers designed an intervention comprising nurses’ adherence to a care bundle checklist and an educational campaign for the care-taking team and applied it in the second period. Patients either accidentally removed the central venous lines secondary to agitation (47%), or it happened by loss of catheter securement (21%), or during daily care (17%) or patient transfer (13%). Such inadvertent incidents resulted in reinsertion with another central venous line (69%), agitation due to sedation interruption (47%), development of hemodynamic instability because of interruption of inotrope administration (30%), significant bleeding that required intervention (21%), and no complications (39%). The overall nurses’ compliance to the care bundle checklist improved from 87% to 97% after introduction of the intervention and the number of devices found in place increased. Therefore, the designed care bundle checklist and educational program successfully decreased the accidental removal of critical care devices.
Working in the intensive care unit (ICU) is stressful because of the critical medical conditions managed therein that warrant important decisions and could have serious implications. Furthermore, taking care of critically ill patients with different needs adds to this stress because the treatment of such patients extends beyond standard care to assigning additional importance toward avoiding complications and possible adverse events. One such important event is the accidental removal of devices including life sustaining devices such as Endotracheal tubes or supportive devices such as NGT and central venous catheters. It is a relentless concern of critical care staff to avoid such preventable events that can alter the course of a patients’ stay in the department. In order to start a project aimed at decreasing these incidents, we found it paramount to first understand the possible causes of such events and then identify the practical interventions needed to reduce their likelihood of occurrence. We collected six months’ data of the common devices accidentally removed and the relevant clinical information of the patients concerned. After dissecting the etiology and confounding factors, we designed an educational program including lectures and orientations targeting the ICU staff to improve their knowledge of the subject and a care bundle checklist for the nurses to comply with for each patient. Our aim was to assess the nurses’ compliance to the bundle form and to assess if this compliance impacted the incidence of accidental device removal.
A) Study population and sampling:
This audit was conducted in the Adult Critical Care Department of King Saud Medical City, Riyadh, Saudi Arabia, all adult patients (age >18 years) admitted to the hospital and had a device inserted were included in our study, there was no sampling process as our target was to recruit as much patients as we can. No inclusion or exclusion criteria had been applied.
B) Study objective and variables:
The aim of this audit was to check the nurse compliance to accidental removal of device bundle checklist, and to determine if the adherence to this bundle and our training sessions will impact the incidence of device removal.
The prevention of accidental removal of devices checklist (care bundle checklist) that we followed was composed of two parts. The first part was regarding the risk factors of device removal and included the following criteria:
The second part was regarding precautionary measures that prevent accidental device removal if a patient has two or more of the abovementioned risk factors; it was composed of the following elements:
To determine the incident of device removal and its risk factors and complication another form was used. This form had 3 components as following:
C) Study period and data collection:
The study involved two six-month consecutive periods; the first was from August 1, 2019 to January 31, 2020, and the second was from February 1, 2020 to July 2020. Data from the first period included the files of patients who experienced accidental device removal; these were reviewed retrospectively. In the second period, we conducted a prospective analysis of the bundle forms (care bundle checklist) during and after our educational campaign, which consisted of lectures, presentations, and daily clinical rounds.
D) Work and intervention:
The target of our campaign was to increase the nurses’ compliance to the care bundle checklist to 100% and to decrease the incidence of preventable critical care device removal to zero. Our strategy consisted of a series of lectures for all ICU staff by the Quality Department team, a daily assessment conducted by the nurses-in-charge to ensure the compliance of bedside nurses to the care bundle checklist, the submission of a weekly report to the campaign committee regarding the nurses’ compliance to the care bundle form, the establishment of a call center run by personnel from the Quality Department who answered any query concerning the care bundle, and a monthly analysis of the data to detect any discrepancies to make corrections accordingly.
E) Statistical analysis:
The collected data entered in excel sheet. A simple statistical analysis was performed by excel program. The frequency of accidental device removal during the audit period and the major outcomes of such events were determined. Frequency and percentage of each risk factors also described. Finally, the number and percentage of the nurse’s compliance with the care bundle checklist before, during, and after the campaign were calculated.
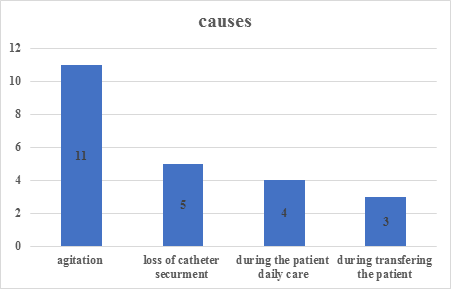
As seen in Figure 1, the vast majority of accidental central line removals were done by the patients themselves secondary to agitation (47%). Accidental critical care device removals because of loss of catheter securement, or during daily care or patient transfer were 21%, 17%, and 13%, respectively.
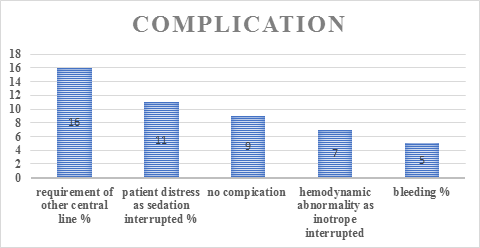
Most patients (n=16/23, 69%) with accidental central venous line removal required another device insertion (Figure 2). Other most common complications of accidental removal of central venous line were agitation due to sedation interruption (47%), development of hemodynamic instability because of interruption of inotrope administration (30%), and significant bleeding that required intervention (21%). No complications were seen in 39% of the patients.

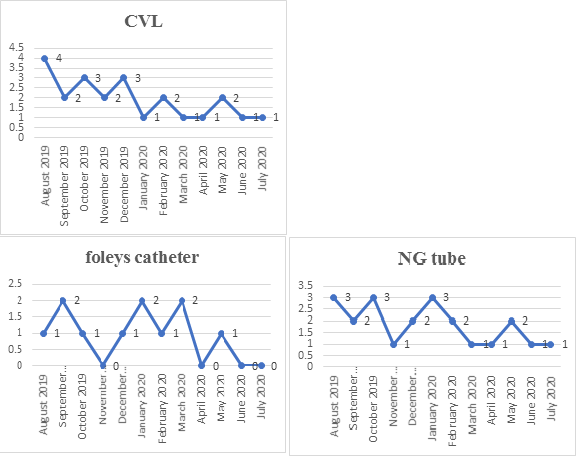
The overall compliance to the care bundle checklist improved from 87% to 97% after introduction of our intervention (Figure 3). Additionally, the compliance to each individual element of the checklist improved except for the requirement of 1:1 nurse to patient ratio that could be attributed to a staff crisis during the surge of coronavirus disease cases. Figure 4 shows the trends of accidental removal of three critical care devices evaluated during the study.
As seen in Table 1, there was a marked improvement in the number of critical care devices in place, during and after the intervention.

Different devices and catheters attached to patients are necessary in critical care departments. However, they may incur various complications and side effects related to their insertion or accidental removal. Such adverse events are important to discuss, as they are largely preventable. In our study, we show that accidental removal of critical care devices can be prevented by proper training and education of the care-taking staff. Our study also highlights the importance of complying with a care bundle checklist that addresses common causes of accidental removal of critical care devices such as lack of proper sedation.
In particular, the dislodgement rates of central venous catheters have been estimated at 1.8%–24.5%, with greater than five million catheters dislodged per year [1-5]. In our hospital, this incidence was 8.9% (table
1) and was of notable importance considering the potential increase in risk of morbidity and mortality it entails [6] in addition to other implications such as prolonged hospitalization, insertion of other venous catheters and related complications, and further financial burden [7]. Moreover, our observations revealed specific complications such as hemodynamic instability in 30% of the patients (Figure 2). Several factors were associated with and could possibly cause the accidental dislodgement of the venous catheters; the most common contributors were patient agitation (47%) and loss of central line securement (21%; Figure 1).
With the possible causes and contributors in mind, we started daily lectures and weekly presentations, targeting the ICU staff on the importance of avoiding these kinds of events and equipping them with knowledge regarding the management of patients who have different critical care devices attached to them. Furthermore, we added the care bundle checklist in every patients’ file and ensured that it was discussed and presented in the daily clinical rounds.
Our main target audience for the educational activity were the nurses, as we believe that they have a major role in patient management and have the longest contact time with the ICU patients. Therefore, it was important for the care bundle to be implemented and designed based on the nurses’ needs, and experiences. However, we also wanted this effort to involve the entire team taking care of the patient so we emphasized the importance of a multidisciplinary approach involving respiratory therapists and physicians; extensive evidence suggests that this is the most effective way to obtain better results [8, 9].
After implementing these measures, we analyzed the findings and found a remarkably positive result (Figure 3 and 4). There was a notable improvement in the rate of nurses’ compliance to the care bundle checklist that translated into a clear reduction in the accidental removal of critical care devices, such as central venous catheters, Foley catheters, and nasogastric tubes (Figure 3).
Dislodgement of life-saving devices have serious consequences in critical care departments and efforts should be made to decrease the incidence of these preventable events. Addressing the possible causes and designing a care bundle checklist, which ensures compliance to prevention measures, in addition to a targeted training of the care-taking staff could lead to satisfactory results that translate into better patient management.
No conflict of interest.
No funds provided to this work
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
